Introduction
Hospital-acquired infections (HAIs) remain one of healthcare's most persistent challenges. On any given day, approximately 1 in 31 hospital patients has at least one healthcare-associated infection, contributing to roughly 687,000 HAIs annually in U.S. acute care hospitals and approximately 72,000 deaths.
The financial toll compounds the human cost—the five most common HAIs cost the U.S. healthcare system nearly $10 billion annually.
In response, hundreds of health systems globally have deployed cleaning robots to address the gaps that manual cleaning cannot reliably close. These machines—UV disinfection units and autonomous floor scrubbers—operate where human cleaning protocols consistently fall short. The global disinfection robots market was valued at $3.60 billion in 2023 and is projected to reach $12.79 billion by 2030, exhibiting a compound annual growth rate of 19.2%.
This guide explains exactly how UV disinfection and autonomous cleaning robots work in practice—their mechanisms, deployment stages, and documented outcomes.
Key Takeaways
- Two main types: UV-C disinfection robots that destroy pathogens, and autonomous floor scrubbers that remove physical contamination
- UV-C robots emit short-wavelength ultraviolet light (200-280 nm) that damages bacterial and viral DNA/RNA, preventing replication
- These robots supplement—never replace—human EVS staff, acting as a second layer of protection after manual cleaning
- Deployment cycles vary: standard patient rooms require ~15 minutes, while operating rooms may need 20-45 minutes depending on the technology
- Adoption is expanding beyond hospitals into airports, hotels, and other high-traffic commercial facilities
What Are Hospital Cleaning Robots?
Hospital cleaning robots are autonomous or semi-autonomous machines designed to disinfect surfaces, clean floors, or perform both functions—reducing pathogen load in clinical environments with minimal human intervention during operation.
Manual cleaning, even when performed correctly, cannot guarantee contact with every surface. EVS staff may miss high-touch areas, and human fatigue introduces variability across shifts. Automated disinfection adds a consistent secondary layer that doesn't tire, rush, or skip.
These are not surgical robots, diagnostic devices, or patient-care machines. They are environmental services tools focused entirely on surface hygiene and infection prevention.
Two Primary Categories
1. UV-C Disinfection Robots These units use pulsed or continuous ultraviolet light to neutralize pathogens on exposed surfaces. They target bacteria, viruses, and spores by damaging pathogen DNA at the cellular level—no chemicals required. Cycle times typically range from 10 to 45 minutes depending on room size and contamination risk.
2. Autonomous Floor Scrubbers These robots use sensors and mapping technology to clean floors without a human operator. They handle physical contamination through mechanical scrubbing and chemical action, using onboard sensors to navigate around obstacles and reduce water and detergent waste.
Understanding how each category works in practice helps facilities decide where to deploy them—and why combining both often delivers the strongest infection prevention results.
How Do Hospital Cleaning Robots Work?
Hospital cleaning robots fall into two categories: UV disinfection robots and autonomous floor scrubbers. Each works differently, targets different types of contamination, and fits into EVS workflows in its own way. Here's how both operate in practice.
Activation and Setup
UV Disinfection Robots: An EVS staff member manually cleans the room first—this step is non-negotiable. The staff member then positions the robot in a designated location within the room and activates a disinfection cycle. Activation can be manual (keypad/remote) or semi-automated depending on the model.
Autonomous Floor Scrubbers: Operators program routes and schedules using onboard mapping software or facility management systems. Once programmed, the robot executes cleaning runs without continuous human guidance, navigating hallways, lobbies, and patient areas independently.
Core Disinfection Mechanism (UV-C Robots)
The photochemical principle: UV-C light operates in the 200–280 nanometer wavelength range. When this light penetrates the cell walls of bacteria, viruses, and spores, it disrupts their DNA or RNA by forming cyclobutane pyrimidine dimers. These dimers prevent normal base pairing, so the pathogen cannot replicate—effectively rendering it inactive without chemical agents.
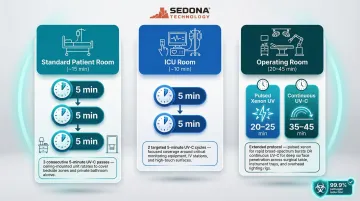
What happens during a cycle: The robot emits pulsed or continuous UV-C bursts that sweep across all exposed surfaces in a room—walls, bed frames, equipment, floors. Cycle durations vary by room type:
| Room Type | Typical Cycle Duration | Notes |
|---|---|---|
| Standard patient room | ~15 minutes | Three 5-minute cycles (both sides of bed + bathroom) |
| ICU room | ~10 minutes | Two 5-minute cycles |
| Operating room | 20-45 minutes | Two 10-minute cycles (pulsed xenon) or single 30-45 minute cycle (continuous UV-C) |
Henry Ford Health System deployed 20 Xenex robots using these standardized protocols across their facilities.
The key performance variable: UV-C effectiveness is directly tied to line-of-sight exposure. Surfaces blocked by furniture, curtains, or equipment receive less UV energy. This is why room setup and robot repositioning within a single room are critical steps. Studies show UV-C achieves >4 log reductions in direct line-of-sight, but efficacy drops significantly in shadowed areas.
Navigation and Autonomy (Floor Scrubbing Robots)
Autonomous floor scrubbers map hospital environments using LiDAR, 3D cameras, and onboard sensors. They detect obstacles, avoid people, and follow pre-programmed cleaning paths through lobbies, hallways, operating rooms, and clinics.
Two operational benefits stand out in real-world deployments:
- Water and chemical savings: Tennant's ec-H2O technology saves 8,730 gallons of water over five years by converting water into a cleaning solution electrically, sharply cutting chemical use.
- Labor reallocation: Bolingbrook High School recovered 20-30 staff hours per week after deploying Tennant T7AMR robots, freeing EVS staff for electrostatic disinfection tasks.
Safety Controls and Monitoring
UV-C robots: Safety mechanisms prevent UV robots from operating when people are present. Motion sensors, door interlocks, and automatic shutoff features ensure UV-C exposure is limited to unoccupied rooms only. This prevents accidental exposure to UV-C light, which can cause skin and eye injuries.
Floor scrubbers: Obstacle detection algorithms cause the robot to pause, reroute, or stop when a person or object enters its path. This enables safe operation in active hospital corridors without disrupting patient care or staff workflows.
Where Hospital Cleaning Robots Are Used
Primary Deployment Zones Within Hospitals
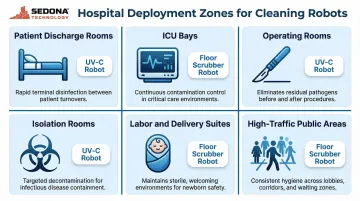
UV-C robots and autonomous scrubbers are deployed across a range of hospital environments, each with distinct disinfection demands:
- Patient discharge rooms — UV-C robots run after terminal cleaning to ensure the next patient enters a pathogen-reduced space, reducing transmission of drug-resistant organisms.
- ICU bays — Intensive care units house highly susceptible patients and hard-to-clean equipment. Studies show pulsed-xenon UV significantly reduces MRSA and drug-resistant Acinetobacter incidence in ICUs.
- Operating rooms — ORs need rapid, verifiable disinfection between cases. Xenex robots can run 2-minute cycles between surgical cases to reduce vegetative bacteria, or 20-minute terminal cleans at night.
- Isolation rooms — CDC and APIC guidance calls for enhanced terminal cleaning in rooms where patients with known MDROs or C. difficile have been treated. UV-C covers high-touch surfaces that manual cleaning may miss.
- Labor and delivery suites — Consistent disinfection protocols here protect newborns from early-onset infections and reduce maternal exposure to hospital-acquired pathogens.
- High-traffic public areas — Lobbies, elevator banks, and waiting areas benefit from autonomous floor scrubbers that maintain cleanliness without disrupting patient and visitor flow.
Conditions for Best Performance
Not every environment is equally suited to robotic cleaning. These systems perform best in:
- Large facilities with predictable room layouts
- Consistent cleaning schedules
- Trained EVS staff who integrate robot cycles into their workflow
Limitations exist in highly variable or cluttered environments where line-of-sight is compromised or navigation is obstructed.
Expansion Beyond Hospitals
The autonomous cleaning technology hospitals pioneered is now being adopted in airports, hotels, shopping malls, and office buildings facing similar hygiene and labor efficiency demands.
For facilities exploring this transition, Sedona Technology supplies UV and autonomous cleaning robots with sales, rental, and leasing options. Free installation and training are included, which lowers the barrier to entry for both large health systems and mid-sized operations.
Benefits and Limitations of Robotic Cleaning in Healthcare
Evidence-Backed Benefits
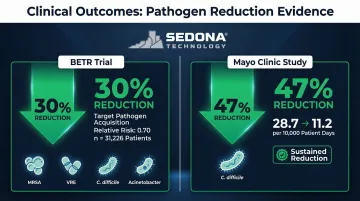
HAI reduction: The landmark BETR cluster-randomized trial demonstrated a 30% reduction in target pathogen acquisition when UV-C was added to standard cleaning. The study involved 31,226 patients across multiple centers and showed a relative risk of 0.70 (p=0.036) for acquiring MRSA, VRE, C. difficile, and Acinetobacter.
Specific pathogen reductions: A Mayo Clinic study achieved a 47% sustained reduction in C. difficile infections (from 28.7 to 11.2 per 10,000 patient days, p=0.03) using pulsed-xenon UV robots after terminal bleach cleaning.
UV-C robots also eliminate the variability that plagues manual disinfection. Every cycle delivers the same UV dose to exposed surfaces regardless of staff fatigue or technique — something no manual process can guarantee.
The Most Significant Limitation
UV disinfection robots are a supplement, not a replacement. They only work on exposed surfaces after manual cleaning. Their effectiveness is contingent on the quality of the human cleaning step that precedes them.
Facilities that deploy robots as a substitute for thorough manual cleaning do not see the expected results. Organic soil (dirt, bodily fluids) blocks UV light, rendering the technology ineffective without proper pre-cleaning.
Operational and Financial Considerations
Before deployment, facilities typically plan around three factors:
- Acquisition model: UV robots are available for outright purchase, rental, or leasing. Costs vary by robot type and room throughput requirements, so most vendors provide facility-specific quotes rather than list pricing.
- Staff training: EVS teams need 2–8 hours of training on room setup, robot positioning, and cycle selection — typically completed before go-live.
- Protocol integration: Robots slot into existing terminal cleaning workflows, but this requires upfront coordination between EVS leadership, infection prevention, and facility operations.
None of these are blockers. Addressed early in the planning process, they're what separates a smooth deployment from one that underperforms.
Conclusion
UV disinfection robots destroy pathogens through photochemical action on exposed surfaces, while autonomous scrubbers handle physical contamination. Together with trained EVS staff, they form a layered cleaning system more effective than any single method alone.
Facilities that understand how these robots actually work — their mechanisms, dependencies, and limitations — can deploy them where they deliver the most impact. That means integrating them into existing cleaning protocols rather than treating them as standalone solutions, and pairing them with staff training to close the gaps that automation alone cannot address.
Frequently Asked Questions
Which type of robot is used to clean and disinfect hospital rooms?
Two main types are used: UV-C disinfection robots (which eliminate pathogens on surfaces using ultraviolet light) and autonomous floor-scrubbing robots (which handle physical floor cleaning). Many hospitals use both as complementary tools in a layered infection prevention strategy.
How long does a UV disinfection cycle take in a hospital room?
A standard patient room typically requires three 5-minute cycles (approximately 15 minutes total) targeting different areas. Operating rooms may require 20–45 minutes depending on the technology and room complexity.
What pathogens can hospital cleaning robots eliminate?
UV-C robots are effective against a broad spectrum of pathogens including SARS-CoV-2, MRSA, C. difficile, VRE, and other drug-resistant organisms. Effectiveness depends on proper exposure duration and line-of-sight contact—shadowed surfaces receive significantly lower doses.
Can cleaning robots replace human janitorial staff in hospitals?
No. UV robots only work after manual cleaning is complete, and human EVS staff remain responsible for setup, quality control, and areas the robot cannot reach. These systems are tools that support your team, not substitutes for it.
How much does a hospital cleaning robot cost?
Purchase pricing varies by robot type and is typically quote-based — UV disinfection robots and floor scrubbers sit at different price points. Facilities can also choose rental or leasing rather than outright purchase, with rental periods starting at two months for lower upfront commitment.
Is it worth buying a hospital cleaning robot?
Facilities with high patient turnover, documented HAI challenges, or labor constraints tend to see strong ROI through reduced infection rates and consistent cleaning quality. Smaller or lower-acuity settings may find rental or leasing a more flexible starting point to evaluate effectiveness before committing to purchase.